

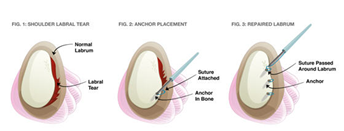
When patients have repeated episodes of dislocations or subluxations (or half dislocations), often times the labrum is torn. This is the fibrocartilaginous rim that attaches normally to the edge of the shoulder joint socket, thereby deepening the joint. When torn, the patient may experience feelings of the shoulder being loose or insecure. There is no confidence with using the shoulder particularly for overhead and sporting activities. Pain may also be a feature.
When a tear is confirmed on MRI scan, there is an option of repairing the labrum arthroscopically. In these cases the labrum, tears off the bone and is repaired back to the joint edge with sutures attached to bone anchors inserted into bone. These anchors may be metal, plastic or dissolvable. Where the capsule (or lining of the shoulder) has stretched this may also be tightened.
SLAP tears are tears of the labrum at the top of the joint where the biceps tendon attaches. In young people, repair can be possible but in older patients the bone is sometimes weak and cannot hold the bone anchors. In such cases we may need to debride the labral tear and release or reposition the biceps tendon.
You are in hospital overnight and in a sling for 6 weeks. After that, an exercise program is commenced and physiotherapy may be required for 6 months. Sport and heavy lifting must be avoided for 6 to 9 months.
The success rate of such surgery after 1 dislocation is about 95 per cent, but if you have had 2 or more dislocations then the success rate drops to about 90 per cent. In persons who have had several dislocations and are likely to resume contact sport an "open stabilization" may be more successful. People who have a hypermobile shoulder with significant generalised ligamentous laxity may be better suited to "open surgery" in selected cases. If you have had subluxations or "half dislocations", arthroscopic surgery is usually very successful. Where there is a SLAP lesion only, surgery is 90 per cent successful.
 Dr. Leonard kuo
Dr. Leonard kuo