

Supracondylar fractures are the second most common limb fractures in children and constitute 80% of elbow injuries. The majority occur within the first decade, with 98% being of the extension type. Gartlands classification is useful as a guide to treatment and alerts us to the potential complications.
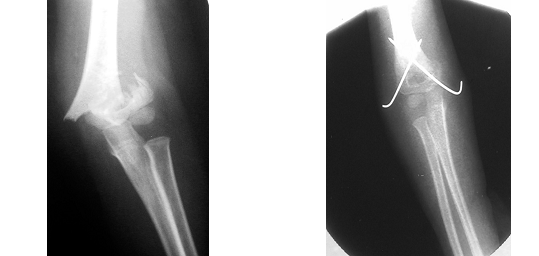
For completely displaced fractures (grade 3), closed reduction and splintage has an unacceptable failure rate. The results of traction are generally good but the main disadvantage is prolonged hospitalisation and cost. Closed reduction with percutaneous K wire fixation produces equally good results with low complication rates and is accepted as the treatment of choice. Medial and lateral crossed pinning is the most torsionally stable configuration. Open reduction is sometimes necessary for irreducible fractures, open injuries and those associated with vascular trauma. Exploration via a medial or lateral incision is preferred to the posterior approach.
Fractures that present later than 2 weeks are best accepted and a corrective osteotomy performed once union has been secured. A well known sequelae of supracondylar fractures is cubitus varus. This is due to a combination of coronal tilt, saggital angulation and horizontal rotation. Beware of the medial column greenstick fracture which may also produce this deformity. The main concern is one of cosmesis and minimal functional loss is seen. Osteotomy is effective treatment.
Fractures that present later than 2 weeks are best accepted and a corrective osteotomy performed once union has been secured. A well known sequelae of supracondylar fractures is cubitus varus. This is due to a combination of coronal tilt, saggital angulation and horizontal rotation. Beware of the medial column greenstick fracture which may also produce this deformity. The main concern is one of cosmesis and minimal functional loss is seen. Osteotomy is effective treatment.
Neurological injury occurs in 7% of cases. Most are neuropraxia and recover fully within 2 months. Posteromedial fractures may be associated with radial nerve palsy whereas posterolateral fractures tend to injure the median nerve and brachial artery. Significant vascular trauma is seen in <1% of cases. The main concern is Volkmanns ischaemia and gangrene. The presence or absence of the radial pulse is an unreliable danger signal. It is more important to evaluate clinically the dynamic function of the forearm muscles. Treatment principles include early exploration, fracture stabilisation and compartment decompression.
Flexion supracondylar fractures are caused by a fall directly onto the elbow. The ulnar nerve is more likely to be injured. Complete fractures can be hard to reduce and require open reduction. Elbow flexion is slow to return.
 Dr. Leonard kuo
Dr. Leonard kuo